“A Blood Test Saved My Life” says young cancer patient

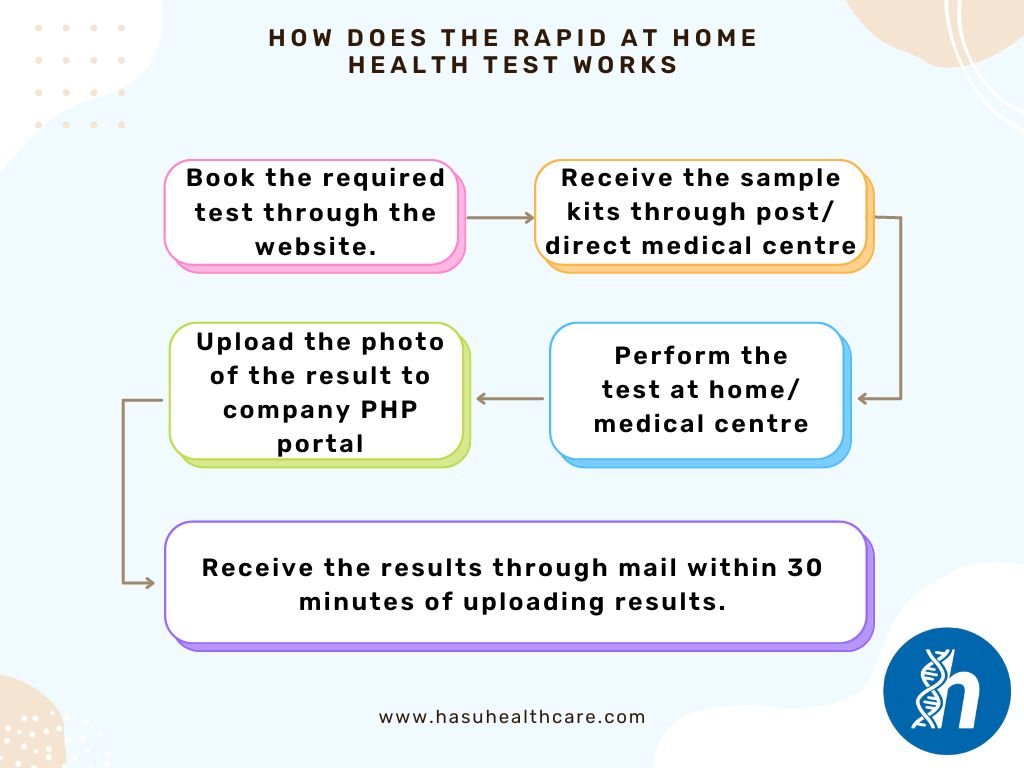
- If your test is Rapid and you have booked and tested at Medical Centre you will your test results in 30minutes after your test , A clinical staff will provide you verbal outcome of your test.
- If you test is run through the postal then a clinical team will call you or sent you an email after received your sample by post and laboratory has performed the test.
- For fit to fly RT-PCR or Antigen test the result will be sent to you by your email as a PDF copy, please check your email inbox, junk box or spam folder the email comes from Hasu Health care.
- Result times vary depending on the test that has been booked.
• The Rapid test has over greater than 96 % sensitivity and 99% specificity for the Biomarkers, the Rapid test tells you whether you have enough level of the Biomarkers or not as Qualitative test. And in most of cases that information is sufficient to alert you for the condition at early stage to start the necessary measures to prevent your conditions to develop further.
MIND you the RAPID test is ALERT you for the under lying conditions you may be unaware of.
We will provide the Diagnosis of the test you have performed and provides you suggestions, the most common suggestion is to contact your GP or your Doctor and ask them that you have run the Rapid test and needs the further investigation.
You can ask our GP service which is Chargeable for £40 per consultation which can be 15 minutes call.
- With postal services they can normally take up to 48 Hours (2 working days) to arrive at our medical centre. (Note the tracking number given on the return label).
- Following table provides overview of the expected results of the postal samples

- Please note that postal services are not operational on Sunday and Bank Holidays, we may receive the kits from the next working day onwards.
- You can organise your own courier/postal service. Postal address is given on the blue card.
- Yes you can with Our Barclay Card Payment system you can Pay using Credit/Debit Card.
- The order number is the Reference to your Purchase which you would receive in your email After the Payment of the test as a Order confirmation email
- The test barcode is Reference to your Sample which is found on the Sample tube and corresponding cards that are sent to you
- For the Preparation of sampling
- Wash or sanitise your hands.
- Follow the Instruction provided on back of the Blue Test Card
- Place the Sample tube back into the box with the Registration Card (purple card) and Keep with you the Blue Test card for your reference
- Stick the provided prepaid Royal Mail returns label onto the return bag.
- Post in a Royal Mail Priority Post Box only.
- Please see our Refund Policy